The Sunday New York Times Magazine’s May 15 “Health Issue” really GOES THERE. Informative unflinching articles cover breast-reduction surgery (as a feminist issue), Brazilian butt-lifts (the women who have them and the women who take care of the women who have them), gender-affirming phalloplasty (reported by a trans-identified journalist, which makes a huge difference), and a straight cismale’s experience with the weight-reduction app Noom. These excellent articles follow on the heels of last week’s cover story by the scrupulous, ever-deep-diving journalist Susan Dominus on how war has turned Ukraine’s booming surrogacy business into a logistical and ethical nightmare for surrogate mothers, their existing families, and the families anxiously awaiting new arrivals in the midst of this unpredictable conflict. The New York Times doesn’t always live up to its reputation as the gold measure for American journalism — its recent lame portrait of late Mayor Ed Koch’s sad love life as a closeted homosexual rightfully drew the fury of observers who remember just how Koch’s destructive homophobia impacted New York City’s response to the AIDS crisis — but then sometimes, like this week’s magazine, it does.
photo by Naila Ruechel for the New York Times Magazine
When I started writing my book THE PARADOX OF PORN several years ago, I was aware that almost everybody I know looks at some version of porn on a regular basis but we hardly ever talk about it. And I get that. Looking at porn – really, anything related to sex – is quite personal and intimate and individual. You don’t reveal your habits to just anyone. Nobody wants to be shamed or judged for their habits or their preferences or their pleasures. Gay men have been shamed and judged enough in their lives. At the same time, stuff that doesn’t get talked about can reinforce shame and inhibition and ignorance, so it’s a bit of a dilemma.
Personally, I love talking about sex, and in my life as a sex therapist and pleasure activist I do a lot of that. I will say that the only context in which I’m interested in talking about sex and pornography is one of complete lack of judgment, led by curiosity and pleasure and shared interest. As the saying goes, “Don’t yuk my yum.”
One of the main skills that a therapist has to cultivate is the ability to make the space safe for people to talk about intimate, personal, sometimes scary, sometimes shameful stuff. When you do that, it’s amazing what insights and self-knowledge and self-acceptance can emerge. As a sex therapist, I’m pretty much required to ask people detailed personal questions about their sexual histories, including their experience of pornography. And once it’s been established that they’re safe to talk freely about pornography, clients open up and I learn fascinating things about what they look at, what they search for, how they first encountered pornography. Guys will mention their favorite porn stars, often rattling off lists of people I’ve never heard of – and of course I Google the names afterwards. You know, professional research! Continuing education!
Writing the book and talking to people about it after it was published also gave me a chance to consider my own history with porn, what I like and don’t like, where I started and where I am now. You may or may not remember the period of time in the 1980s when there was a huge uproar about government arts funding and objections to artists whose work had “homoerotic” elements. Those culture wars haven’t completely come to an end, but it seems pretty silly, considering the more important things to worry about. But I’ll never forget seeing a show by the downtown performance artist Penny Arcade who proudly stated, “I need a little homoerotica to get me through the day.” I could relate! And I think it’s still true!
There was a time when “looking at porn” meant viewing commercial movies, videos, and magazines showing buff hot guys getting it on. With the advent of the internet and smartphones and social media, now there are nine zillion different ways to encounter and enjoy erotic imagery. When I get up in the morning and check my email, I’m likely to find an email from a guy in Hawaii who publishes the “gRUFF list,” a stash of anywhere from 5 to 60 sexy pics in a multitude of categories. In my “Promotions” folder I will undoubtedly have several emails from sex-toy emporia like Mr. S Leather or Fort Troff, announcements from the Tom of Finland Foundation, and discount offers from porn sites like Naked Sword, Himeros, and Antonio DaSilva, all of them containing tantalizing stills and short clips.
My husband and I have a running text exchange with two other friends we call The Pervs Thread, where the four of chat about everything, occasionally tossing in a sizzling JPEG we’ve come across online. Over my desk I have the Colt Hairy Chested calendar, and the first day of every month I send the Pervs Thread greetings from the model of the month. When I have a few moments to kill – when I’m on the toilet, or waiting for clients to arrive, or winding down at the end of the day – I will often cycle among Instagram thirst traps, gay Twitter, Scruff, and Tumblr. Homoerotic imagery is so built into my day, it’s like the air that I breathe.
Is that a problem? I don’t think so. Sometimes when I’ve gorged on a bunch of hot photos or taken time to watch a Joe Gage porn clip on Naked Sword, I may find myself in a trance and start cruising for sex when half an hour before I wasn’t horny at all. That goes with the territory. At the same time, I had a conversation this afternoon with a friend who said he doesn’t look at porn a lot but when he does it reminds him that, “Oh, I’m a sexual being, and I’ve been neglecting my pleasure body lately.”
Think about what you look at, what you like and don’t like, what it adds to your life, what it takes away. If this is a conversation that interests you, consider signing up for the Body Electric School’s five-week class “The 30-Day Porn Cleanse — The Pause That Refreshes.” Over five Sunday-evening sessions starting January 9, Body Electric’s Craig Cullinane and I will invite you to examine your relationship with pornography in a non-judgmental and supportive environment. This is not about “treating porn addiction” – this course views erotic imagery as a portal to pleasure and self-discovery and offers “the pause that refreshes,” so you can return with mindfulness and choice to the porn-watching practice that serves you best.
Once the realization is accepted that even between the closest human beings infinite distances continue, a wonderful living side by side can grow, if they succeed in loving the distance between them which makes it possible for each to see the other whole against the sky.
There has been a lot of talk about the mental health challenges that everyone is facing during this time of the global pandemic, political unrest, and financial turmoil. I feel it myself, and I witness it in the people that I work with. And I can attest that one thing that really helps is witnessing a public figure speak with real integrity and moral authority, as President Obama did at the funeral of Georgia Congressman and civil rights hero John Lewis. Check it out for yourself.
On this day in 1993, I hung out my shingle and launched the practice I call Body and Soul Work. I was ostensibly offering massage. In my heart I knew I was offering sacred intimacy, a term then virtually unknown outside the world of the Body Electric School and its devotees. Twenty-seven years later, I remain committed to this transformational work. I have had many teachers and have studied numerous additional modalities since then. But today I primarily want to thank the teachers that led me to my practice: Joseph Kramer, Keith Hennessy, Doug Fraser (RIP), Chester Mainard (RIP), and Irene Smith. And much gratitude to the clients who have honored me with their trust and openness, in whose presence I have learned and grown. (P.S. don’t try calling the number on the flyer — I got rid of my landline ages ago!)
Aside from the relief Freud offered to the afflicted, he can also remind the rest of us that we are all troubled souls in one way or another that the seemingly robust and successful types that we envy may, more than anyone, be assailed by feelings of self-doubt and failure. To allow for natural unhappiness in our lives and not berate ourselves for feeling it is to stand against the tyranny of the positive-thinking ethos that surrounds us daily. The gift of therapy is not just to cure the deranged but to point all of us to where we have lost authorship of our stories, bring those reasons to consciousness and thus show us the gentle path to healing.
Pretty much exactly three months ago, the entire world came to a screeching halt. As the covid-19 pandemic made its way into every corner of the world, we entered a period of lockdown, working from home if you can, learning how to protect yourself if you fall into one of the categories of “essential workers.” Everything has changed — eating, sleeping, communicating with friends. We anxiously scour the news for reliable information on this new frightening unpredictable virus. For many people, mental health is a challenge; for almost everyone, the financial picture is alarming and uncertain. And then after the murder of George Floyd by a Minneapolis police officer, we are witnessing a huge reckoning as Americans realize we can no longer avoid addressing systemic racism, police brutality, white supremacy, and racial inequality.
A subject that doesn’t get talked about as much but I know is on the minds of almost everyone I know: when am I going to have sex again? When our personal safety and public health depends on social distancing, wearing masks, and disinfecting everything in sight, what happens to physical intimacy, touch, and mutual erotic pleasure? Gay men of a certain age remember going through these convulsions decades ago, when HIV swept through our world and forced us to change our sexual behavior in order to survive. There are eerie similarities between the HIV/AIDS epidemic and the covid-19 pandemic, in terms of how it feels to live through these crises and make healthy choices around sexuality; there are also stark differences.
There’s a lot we don’t know, and what we do know is subject to constant revision. But I want to share a few resources that have crossed my path, for those who are trying to puzzle their way through this question of how to manage sex during this pandemic.
He cites the expertise of Dr. Julia Marcus, assistant professor at Harvard Medical School:
“In the case of staying home to prevent coronavirus transmission, we need to support people in doing that, but we also need to make sure we’re not sacrificing other aspects of people’s health,” [she says]. Of course, Marcus isn’t advocating that we throw away everything we know about social distancing rules and go back to our pre-COVID lives. “We need to support people in having some pleasure in their lives, enough that they can live through this pandemic in a sustainable way.”
The article also cites Mark D. Levine, chair of the New York City Council’s health committee, who called for an end to the “all or nothing” mentality behind the city’s current approach to distancing.
“Let’s give people the tools to understand that the riskiness of social activities lies on a spectrum. We are staring quarantine fatigue in the face. We need new guidance—and policies—to meet this challenge,” he tweeted. “If we don’t give people the information to choose low-risk activities, they will choose high-risk ones—like house parties, large gatherings in front of bars, or swimming at beaches without lifeguards. (All of which is already happening in NYC.)”
On Tuesday May 26, Jeff Vilensky — the founder of MMX, a New York-based private membership group promoting the benefits of massage and healthy living — hosted a town hall/Zoom meeting on gay sex and harm reduction during the global pandemic. The guest speaker was Dr Demetre Daskalakis, queer health warrior, wisdom spreader, and deputy commissioner for the NYC Health Dept and Division for Disease Control. (Dr. Demetre was part of a team that created a remarkably plain-spoken document, “Sex and Coronavirus Disease 2019 (COVID-19),” that attracted titillated attention from the mainstream media for its frank acknowledgement of gloryholes as a creative method of harm reduction.)
MMX has made the video of Dr. Demetre’s talk available publicly via YouTube:
The 16-minute video is worth watching in its entirety, but the gist of it is contained in a simple traffic-light metaphor of green light, yellow light, and red light.
The Q&A afterwards was not included in the YouTube video, to respect the confidentiality of those who attended the town hall Zoom meeting, but in an email to the MMX membership Vilensky generously summarized the key points of the discussion that followed Dr. Demetre’s talk. With permission, I’m including the entire summary, in the interests of community education.
The Q&A included many different questions. Some specific and some general. Answers by the guest speaker followed a few themes along the lines of risk:
“Risk profile” is knowing and accepting that you may be asymptomatic and pass the virus to someone who is more susceptible to it than yourself. Know the science, stay up-to-date on data points, and use those to continuously evolve your choices. The ideal scenario is following current CDC/NYC Health Dept Guidelines (see links in the video). The “Harm Reduction Scenario” is following your best efforts to safeguard yourself and others. Evaluating the risk of all parties in this context, and make informed decisions based on your data, choices, needs, and desires.
“It’s not perfect, but it’s better than nothing.”
Harm reduction is trying to limit your risk and at the same time limiting the risk of others who are potentially at higher probability of infection. We are human and we are gay men who crave physical connection. Think about what works for you now and the level of risk that you are willing to take, if any. Be judicious and understand the risk spectrum/perspective and where you fall on that spectrum. (The doctor used the example: With regard to jumping off a cliff – Are you completely scared of heights? Or are you a bungee jumper? Where are you along that scale?)
BEHAVIOR: BEING OPEN, HONEST, and UPFRONT
Having frank and open conversations with sex partners about the following is extremely important right now:
– Activity and behavior
– Current exposure
– Symptoms
– Past exposure
– Antibody tests
– Level of risk you are willing to accept
Making decisions based on honest communication is extremely important. It shouldn’t be weird or uncomfortable to talk about COVID (just as you would about STIs). Navigate this world we are in and avoid judgement. Judgement throws the conversation under the rug (shaming, feeling wrong). Everyone needs to feel comfortable enough to participate in open and honest communication.
Sex & Connection:
Prevent as much face-to-face interaction as possible. Stay distanced, or masked, or create a barrier to prevent the travel of respiratory droplets. Eye and face coverings throw the odds in your favor. Continue to use chat and video options. Develop scenes that protect you and your partner. Remember condoms? Incorporate your masks and gear into some fetish play. Be creative. Make it hot.
The virus is primarily transmitted through respiratory droplets. If you keep your distance and use some form of a mask, you are likely at lower risk.
It’s important to have really good hygiene. This means washing before and after any physical contact. You’re going to want to thoroughly clean every part of your body that may have been exposed to droplets. We are learning more everyday, but we don’t think this is sexually transmitted and if it is, it’s a very inefficient transmission method.
Questions for Yourself:
Where does my desire and right to pleasure live versus what my responsibility is to myself, my family, my close circle, and the general community? If you are going to hook up, what does it mean when you leave any encounter and go to another? What’s at stake? Who’s at risk?
Not Recommending:
Gatherings of large groups.
Ignoring warnings and guidelines or throwing caution to the wind.
Not a good idea to “kiss grandma” if you are circulating.
Not a good idea to kiss at all outside your trusted partner.
Antibodies:
There were a lot of questions about those with antibodies and what that means in terms of transmission, reinfection, time lapse before having relations, etc. A very complicated issue.
Having unprotected sex (no masks or social distance) with someone who has the antibodies can give you a higher sense of safety. But there is still not yet enough definitive evidence that people with antibodies are immune from reinfection.
All the health organizations say those who have antibodies for COVID-19 are not necessarily immune. However, the data implies that it seems highly unlikely or rare that a COVID reinfection can occur for most people. We think that COVID-19 infection equals some amount of immunity for some amount of time. However, there is still a lot of uncertainty. There’s no definitive evidence that there is immunity or at least long-term immunity. However, the risk of reinfection for someone who has tested positive is realistically very low and possibly even non-existent.
Many of the antibody tests are not so great. The ones that are FDA-approved and are being done in New York are pretty good but some of them cross-react with other common strains of coronavirus. So a positive antibody test could mean you’ve had another coronavirus, but not COVID-19.
In the case of having sex with your partner: if he’s at least 10 days past his initial signs or symptoms and has not had a fever for 72 hours, the risk of him transmitting the virus to you is very low. This also holds true for the risk of becoming reinfected, which means that it is probably safe for him to have sex again.
Understand all the caveats and uncertainty wrapped around this topic.
HIV Meds:
There is no study that concludes that being on HIV meds confers any specific protection from COVID-19 other than keeping your HIV viral load suppressed. It does clearly look to lower risk of more severe complications from COVID-19 should you contract the virus.
The Beach:
The virus is unlikely transmitted by surfaces, but washing your hands is important. Saline and heat destroy the virus, so it’s not in salt water or hot sand. But the hot guy sitting in the sand next to you that you decide to make out with is a potential risk!
Traveling with others? A strategy to consider is to isolate yourself a few days before you enter into a new scenario.
Creating Connections:
There was a discussion about those creating “pods” or groups that have formed or are forming to become your current “household”. This also can pertain to group shares. The same risks are inherent here given those in your pod will be expanding their contacts and interactions. It goes back to hand hygiene, face coverings, open honest communication, risk assessment, and evolving your own risk profile within the context.
Testing Frequency:
There is some notion to test frequently and we may see this more in the future. Understand the difference between the active “viral” test and the “antibody” test. There are some occupations that are now being told to test once a week or once every couple of weeks. Right now, if possible, getting tested on a regular basis (every 3-4 weeks) may be a good plan. Be sure that if you’re feeling symptoms then you go home and stay home until you get your test results.
The viral test is for a current diagnosis of an active infection. There are 3 types of tests for this: swab up your nose, swab in mouth, spit test.
The antibody test is not for diagnosis. It tells you if you have been exposed in the past. Neither test is perfect!
Anal Shedding:
Not as much data on anal shedding as from nasal shedding. For respiratory and nasal, viral traces can sometimes be present up to six weeks after complete resolution of symptoms. Data for anal is unclear. The test looks for the genetic material, but it does not tell you if the virus is alive or not. The CDC did a study where they swabbed people, many days after they developed symptoms, and what they found is not one human swab had the active, live virus after day 9. So it’s possible to extrapolate this for COVID-19 in feces; that it could be there for a very long time, but it doesn’t mean anything if it’s not living.
Being a Carrier / Asymptomatic:
Most people who have been exposed to COVID develop symptoms within 5 to 7 days (could be up to 14 but rare). Remember, there are people who get exposed who have very mild symptoms or are asymptomatic. Guidance is, if you were to get tested without symptoms, wait for your results or wait 10 days before you go out into the world. You don’t carry COVID-19 for years or months or weeks. You get the infection and then it goes away. There does not appear to be a carrier state for COVID-19. If you had the infection, you should be “done” with it if it’s been 10 days since you first had symptoms and if you haven’t had a fever for 72 hours. However, for people with a weakened immune system it could last up to 21 days. Reinfection may happen but it doesn’t seem to be common or frequent.
Stopping PreP:
One way to go about this is PreP on Demand. Take 2 pills from 2 to 24 hours before you have sex. Take 1 pill 24 hours after that, and another pill 24 hours after that.
STI Clinics and Avail of Testing Sites:
There is a grassroots movement to eradicate / dramatically lower STIs while in the midst of this pandemic. Tomik Dash, an MMX Pro, is one of the founders of sexrev20.org. He asked the doctor when we might see the city’s sexual health workers re-allocated back to their original posts (presumably, testing and treatment in NYC is hard to get at this time). They are looking earnestly at this, as more and more health centers and sexual health clinics are becoming fully operational again. There is currently tele-medicine for sexual health, and the Chelsea and Fort Greene clinics are open for on the phone consultations.
—
Speaking for myself, I appreciate the good work of these health professionals in communicating this information to the public as clearly as possible. If you have further questions, concerns, or resources to share, please don’t hesitate to contact me.
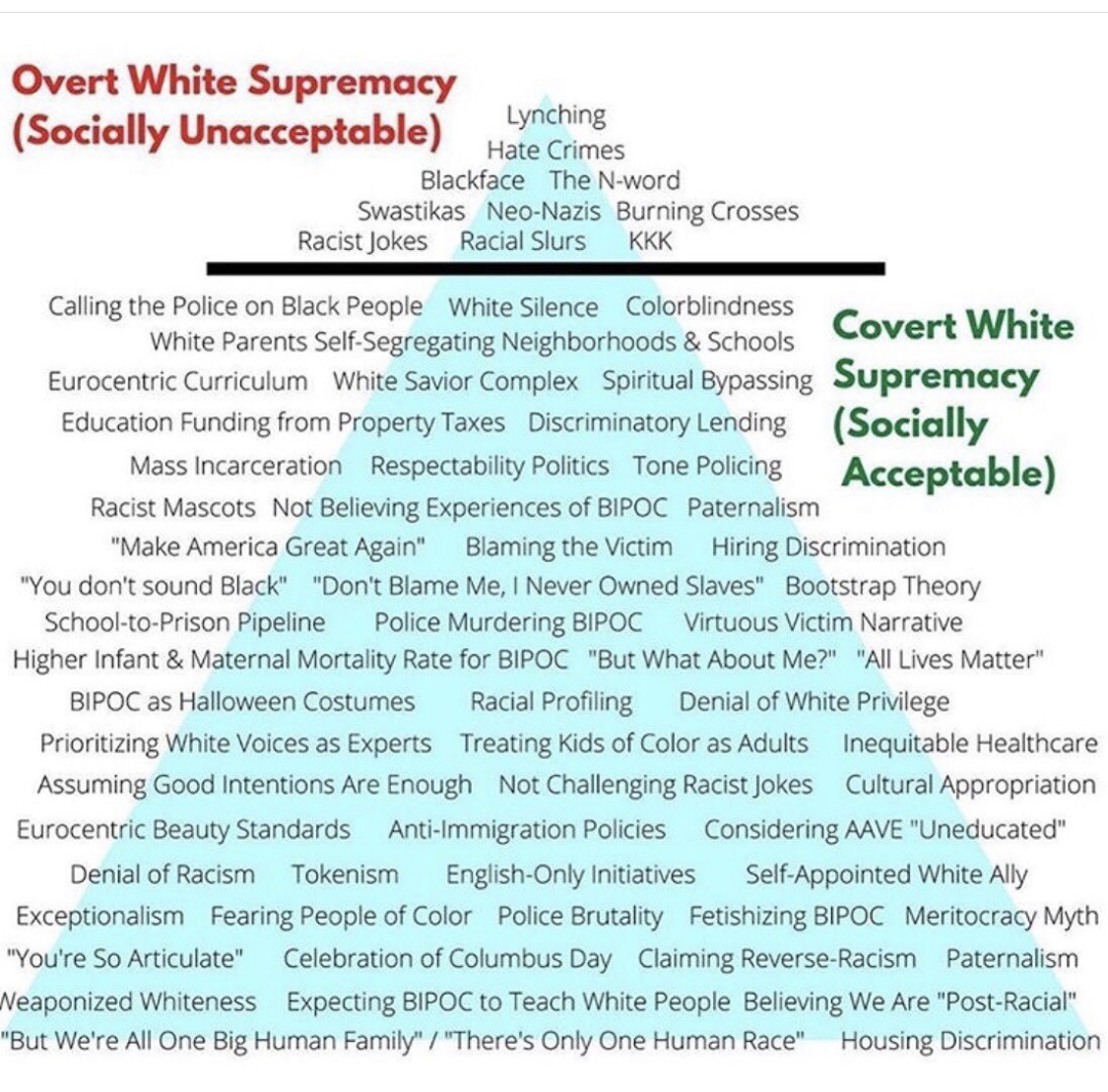
The murder of George Floyd by a Minneapolis police officer is just one (and not even the most recent) incident in a long shameful history of black Americans being treated as if their lives have no value. The video footage of Derek Chauvin kneeling on Floyd’s neck for 8 minutes and 43 seconds has galvanized a worldwide response demanding action, education, and change. There’s lots to do and many choices to make. One place to start is this curriculum called “Justice in June.” This resource was compiled by Autumn Gupta with Bryanna Wallace’s oversight for the purpose of providing a starting place for individuals trying to become better allies.
For white people engaged in anti-racist work, our most important task is to examine our own experiences as white people — how we have been educated, steeped in, benefit from and yet are trained not to notice white supremacy and racial inequality all around us. White people need to talk to white people about this. I’m in this conversation and welcome anyone who wants to join me.
This image was created by Safehouse Progressive Alliance for Nonviolence (2005) and adapted by Ellen Tuzzolo (2016), Mary Julia Cooksey Cordero (2019), and the Conscious Kid (@theconsciouskid on Instagram, 2020).
We’ve all heard plenty of sound advice from medical professionals about what to do to avoid exposure to covid-19 in hopes of not getting sick. What happens if you do get sick? I feel like I’ve read a lot of fairly general instructions, but nothing as specific and clear as this information shared on Twitter by a nurse. I can imagine that many people who have symptoms (or think they might have symptoms, which probably most of us do from time to time) panic a little and everything you’ve heard about what to do next flies out of your head. If that were me, I would be following these guidelines to the letter:
“What I have seen a lot of are recommendations for how to try to avoid getting COVID in the first place — but what I have NOT seen a lot of is advice for what happens if you get it.
You basically want to prepare as though you know you’re going to get a nasty respiratory bug, like bronchitis or pneumonia. Just have the foresight to know it ‘might’ come your way!
1. Things you should actually buy ahead of time:
– kleenex
– acetaminophen (Tylenol)
– whatever your generic, mucus thinning cough medicine of choice (check the label and make sure you’re not doubling up on acetaminophen)
– honey and lemon can work just as well
– vicks vaporub for your chest is also a great suggestion
2. if you don’t have a humidifier, that would be a good thing to buy and use in your room when you go to bed overnight. (you can also just turn the shower on hot and sit in the bathroom breathing in the steam)
3. If you have a history of asthma and you have a prescription inhaler, make sure the one you have isn’t expired and refill it / get a new one if necessary
4. have your favorite soup on hand
5. stock up on whatever your favorite clear fluids are to drink – though plain water is fine; you may appreciate some variety
SYMPTOM MANAGEMENT
a. if you have a fever over 38C / 100.4F, take Acetaminophen rather than ibuprofen
b. hydrate (drink!), hydrate, hydrate
c. rest lots. even if you are feeling better, you may still be infectious for 14 days and older people and those with preexisting conditions should be avoided
d. ask friends and family to leave supplies outside to avoid contact.
You may not NEED TO GO TO THE HOSPITAL unless you are having trouble breathing or your fever is very high (over 39C / 102F) and unmanaged with meds. 90% of healthy adult cases thus far have been managed at home.
I’m assuming you’re equipping yourself with lots of useful information about riding out the covid-19 pandemic in healthy ways. I will post things from time to time that I find especially valuable, in case they haven’t cross your path. Someone shared this video with me that I now play at least once a day, as a way of remembering that however far apart we have to be right now, we can choose to be “for each other.”